
|
|
Needle length - how crucial is it in anaphylaxis? |
|
|
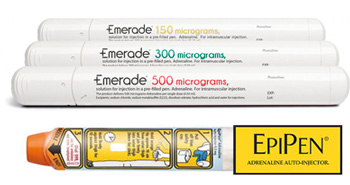
The injection of adrenaline (epinephrine) into the bloodstream via an Epipen or similar device is generally regarded as a life saving treatment if someone suffers an anaphylactic shock as a result of eating a food, ingesting a medicine or being stung by an insect. But there is increasing concern that although the adrenaline/epinephrine can indeed reverse an anaphylactic shock if it reaches the blood stream, in a worrying number of cases it may never do so as the needles used to inject it are too short to reach the muscles which will propel the drug into the bloodstream. Very briefly, when you go into anaphylactic shock the allergen ‘provokes’ a series of chemical reactions that result in a massive release of histamine. This causes angioedema or swelling of the face, the throat and the airways, creating wheeze and, in those who also suffer from asthma, often triggering a major asthma attack. (It is believed that deaths from anaphylaxis over the years may have been seriously under-reported as they were mistaken for straight asthma attacks, rather than anaphylactic reactions.) However, histamine also causes the small blood vessels, or capillaries, to become leaky. So much fluid seeps out of the blood vessels into the cells that there is no longer enough fluid to keep the main vascular blood system flowing, so blood pressure plummets, depriving the major organs of sufficient blood to keep them operational. Adrenaline reverses the symptoms of anaphylaxis by acting on alpha and beta adrenergic receptors in the body. It is always advised that the adrenaline should be injected into the muscle of the outer mid thigh where there are very few nerves, tendons, arteries or veins to hit by mistake. It is also one of the least painful places to inject. But, more importantly, the adrenaline will get absorbed into the system much quicker if it is injected into a major muscle such as the thigh muscle which will propel it round the body much faster than if it is injected into a relatively small muscle in the arm which may only distribute it locally. However, injecting into the thigh has relevance as far as needle length is concerned. Adrenaline injections were originally devised for the treatment of soldiers in battle needing to inject atrophine as a nerve gas antidote. But these soldiers would normally be fit young men with muscular thighs, so problem about the needle delivering the adrenaline/epinephrine directly into their muscles. But these days many of those suffering from serious allergies will not be fit young men but girls or women and even relatively slim women have a much thicker layer of flesh covering the muscles on their thighs than young men – that is the way they are built. So the standard length needles, designed for fit male thighs, may not be long enough too reach the muscle in girls or women and deliver the life saving adrenaline/epinephrine to where it is needed. This has become an increasingly worrisome issue with the death from anaphylaxis of a couple of young girls despite having used their Epipens. Thirteen-year-old Natalie Giorgi, for example, who died from peanut anaphylaxis last year after her father, a physician, had injected her with no less than three doses of epinephrine via three Epipens. It is arguable that her death could have resulted from her father waiting too long to administer the first dose. But it could also have been because, even though Natalie was quite a slim girl, the epinephrine was not getting through the flesh of her thigh to reach the muscle. Back in December 2013, research was already in the public domain suggesting that 'the current epinephrine auto-injector needle length is inadequate for intramuscular injection, especially among women'. (Predictors of epinephrine auto-injector needle length inadequacy American Journal of Emergency Medicine December 2013.) Now new research, presented at the BSACI meeting in September, showed that '68% of our allergy population have a STMD (skin-to-muscle depth) greater than the most common EAIs (epinephrine auto-injectors) putting them at potential risk of EAI failure. The key predictors for increased STMD were female gender and a BMI >30. EAIs require longer needles to ensure IM (intra muscular) administration and ultrasound at point of prescription would aid needle length selection.' This means that 68% of the allergic population may currently be relying on a totally ineffective tool to save them should they suffer from anaphylaxis – an extremely frightening statistic for all women with anaphylactic allergies, for the parents of children with such allergies and for the medical professionals treating them. Although, given the poor level of knowledge and awareness about allergy in primary care, it is very unlikely that the vast majority of GPs are even aware that there is an issue, let alone realise that they should be using ultrasound to determine skin-to-muscle depths and the prescribing longer needles for those who need them. Not that, if they did, that would necessarily help that much: for now, only one auto-injector, Emerade, comes with a longer needle. It may seem bizarre that this should be so when different length needles for heavier diabetics, or for performing acupuncture on those with high BMIs, have been standard for years. None the less, this is currently the case although a recent dictum from the Committee for Medicinal Products for Human Use recommends 'amendments to the product information, in order to reflect the uncertainties in whether a single administration would suffice for any given episode and advise that patients are prescribed two pens which they should carry at all times, to include a recommendation for immediate associates of patients to be trained to use the auto-injectors and to include information on the needle length'. None the less, for now the initiative remains, as is so often the case, with the allergic patient. As Ruth Holroyd of What Allergy?, herself anaphylactic to three different foods, urges: all patients being prescribed auto-injectors must insist on an ultrasound of their thighs and then, if the results suggest skin-to-muscle depth greater than the standard Epipen can reach (7.5-15mm), demand a prescription for an Emerade which has a 25mm needle. For a more detailed investigation of the auto-injector questions, see her blog Why ALL women with anaphylaxis should have an ultrasound.
October 2015 If you found this article interesting, you will find many more articles on anaphylaxis here, and reports of research into anaphylaxis here. |












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}