
|
|
|
| Dr Harry Morrow Brown explores some intriguing cases |
Any experienced clinical or paediatric allergist must have encountered occasional cases where allergy and emotion are inter-related. I present seven case histories which illustrate the remarkable effects allergy or intolerance to food can have on behaviour, and might be of interest to the parents of children with behaviour problems.
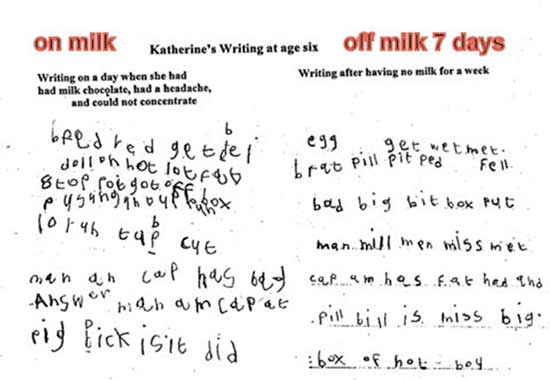
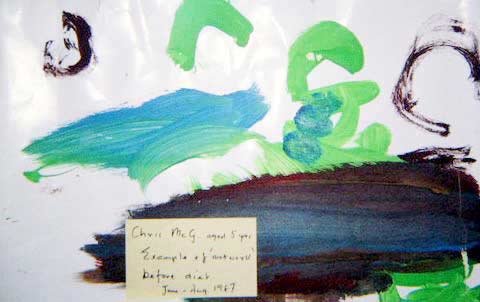
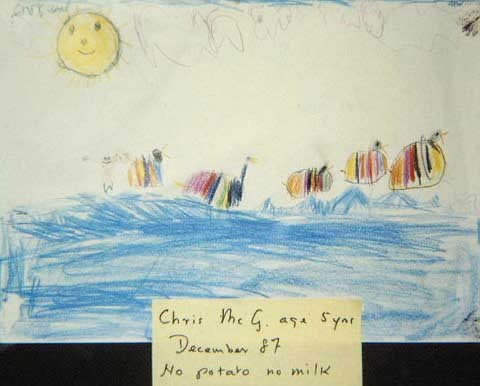
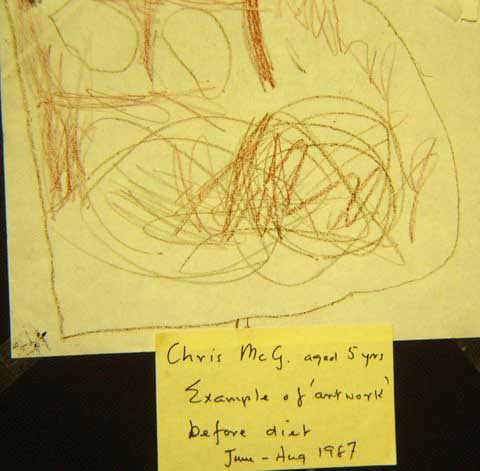
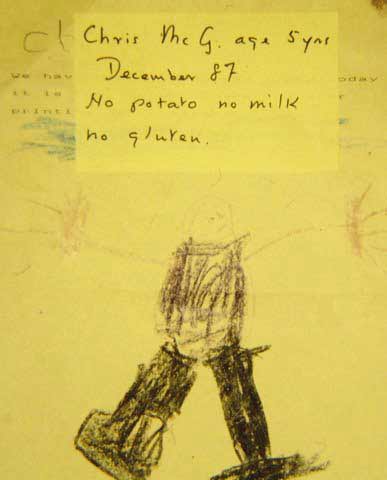
(Ed. See review of the Nutrition and Addiction handbook which includes chapters on both food addiction and chocolate addiction.) Case 2 – Tara Case 3 - Jennifer Case 4 – Paul Christopher was six when first seen, had been bottle fed, with feeding difficulties from the start with frequent vomiting, loose stools, and bloating. As he grew older his behaviour became worse and worse. His mother was sure that his problems were due to food, but a prominent paediatrician considered that the cause was faulty parenting and over-anxiety. She could not accept this and finally was referred to me.
His mother also noticed that the father was always bad-tempered and irritable on arriving home on Friday evenings, and established that this was triggered by having fish and chips on the way home. He did not have potato at any other time, and total avoidance ensured marital harmony. Eventually he was admitted to hospital with asthma and on discharge was referred for allergy investigation aged nine. I found that he was very allergic to the family cats, but he was no better after they were removed. Final comments I have seen many other cases of allergy affecting the brain, but these are the most striking and dramatic examples encountered in over fifty years experience. Unfortunately, in all but two cases it was impossible to follow them up to adulthood, so we will never know what happened to them and whether they finally became normal adults. H Morrow Brown MD FRCP(Edin) FAAAAI (USA) You can reach Dr Morrow Brown via his website at www.allergiesexplained.com First published December 2011
More articles on food intolerance
|












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}